

You know the story. It always starts the same way.
A weird twinge in your shoulder during thrusters. A tight calf that doesn’t quite warm up on the run. A back that feels “off” the day after a heavy deadlift session, but you tell yourself it’s just DOMS. So you tape it, foam roll it, hit some banded pull-aparts, take ibuprofen, and load the bar again on Monday.
Two months later you’re sitting on the physio’s table getting told you’ve had a partial rotator cuff tear the entire time, and the reason you can’t press overhead anymore is because you spent eight weeks training around something that needed to be seen, not pushed through.
Here’s the dirty secret of CrossFit, HYROX and functional fitness: we’re brilliant at training hard and absolutely terrible at gathering data on our own bodies. We track our Fran time to the second. We weigh our oats to the gram. But when something hurts, our default move is “wait and see” – which, in practice, usually means “wait and make it worse.”

This article is the conversation your coach probably hasn’t had with you yet. It’s about knowing when a niggle is just a niggle, when it’s something that needs a picture taken of it, and – just as importantly – when it’s worth scanning yourself before anything hurts, because that’s how high-performing athletes are training in 2026.
Scan.com is the platform that makes that doable for normal humans without a six-figure concierge doctor. Results in days, not months.
Let’s get into it.
The “Train and Hope” Era is Over
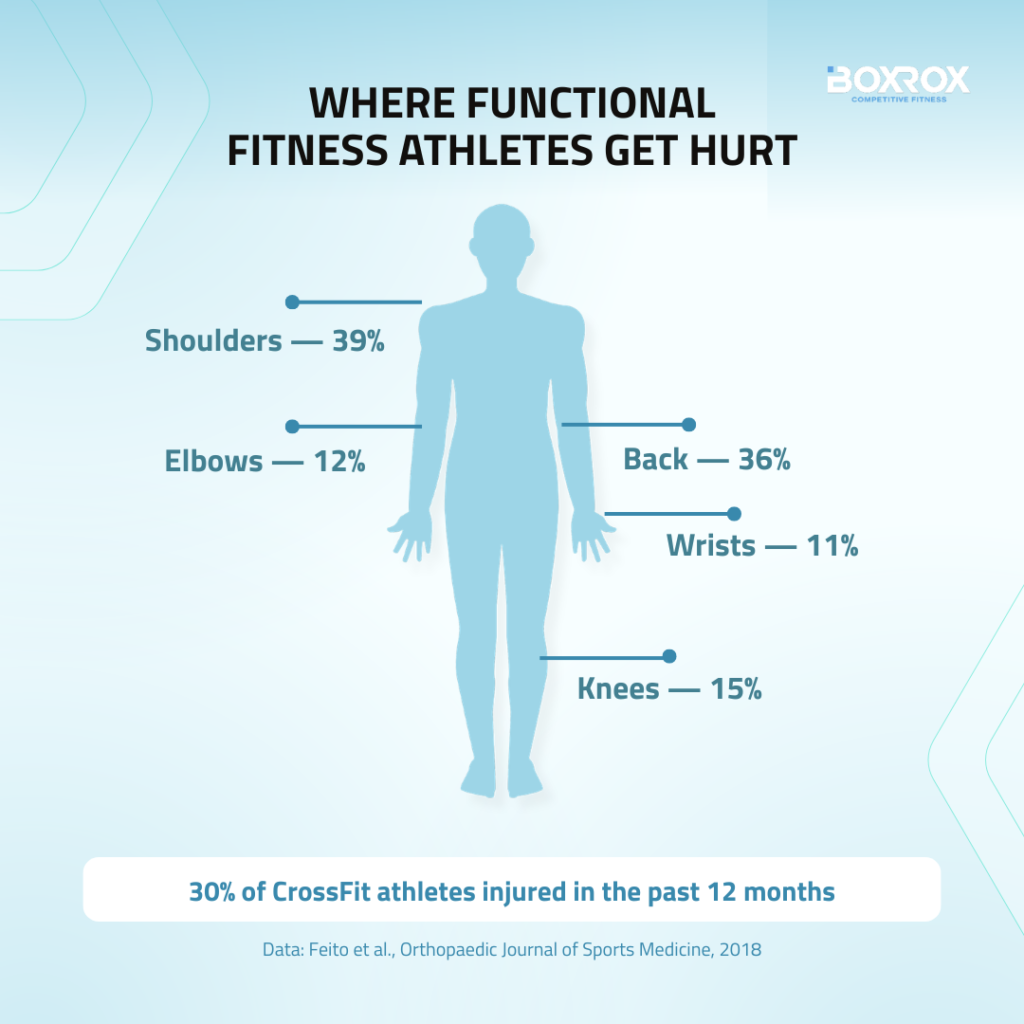
The numbers on functional fitness injuries are not subtle. A four-year study surveying over 3,000 CrossFit participants found that roughly 30% had sustained an injury in the previous 12 months, with the shoulders (39%), back (36%), knees (15%), elbows (12%) and wrists (11%) taking the biggest hits. HYROX physios will tell you the same thing – Achilles, patella, rotator cuff and lower-back issues dominate their clinics, usually showing up as “niggles” that the athlete ramped through.
Meanwhile, NHS diagnostic waiting lists in the UK now stand at 1.8 million people, that’s up 189,000 on January 2025. And a chunk of those wait two months or more for an MRI specifically. In the US, even insured athletes routinely face $1,000+ out-of-pocket costs for imaging once deductibles are factored in.
That’s the bottleneck Scan.com was built to break. Founded in the UK in 2017, the platform now operates across the UK (150+ scanning centres) and the US (live in multiple states). It’s been named one of Europe’s fastest-growing companies in the Financial Times FT1000 ranking – 6th in the Health Care category – and is rated “Excellent” on Trustpilot with 4.4 out of 5 from nearly 4,000 reviews.
The mechanics are simple: search the scan you need, pick a location and time, book online, have a quick clinician video call, get scanned, and get a digital report back – typically within 1–3 days in the US or 7–10 working days in the UK. The report comes with plain-English diagrams, so you don’t have to Google what “supraspinatus tendinopathy” means at 11pm.
1. DEXA: Stop Guessing About Your Body Comp
Smart scales lie. Calipers depend on who’s pinching you. Bioelectrical impedance fluctuates with how much water you drank that morning. If you’re a competitive functional fitness athlete trying to figure out whether your last training block actually built muscle or just made you puffier, you need DEXA.
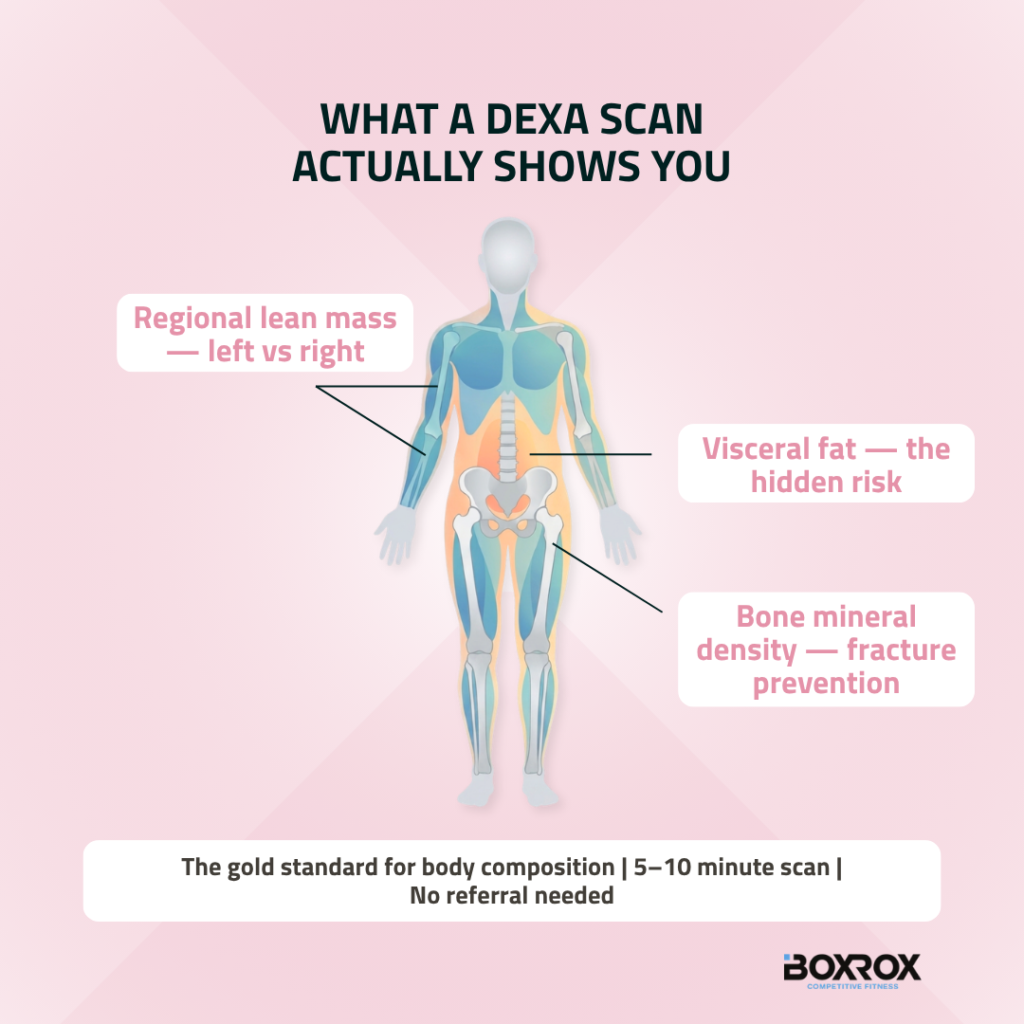
DEXA (Dual-Energy X-Ray Absorptiometry) is the gold-standard reference method every other body-comp tool is validated against. It scans you in 5–10 minutes lying down, and gives you three things no other method does properly:
Regional lean mass – left arm vs right arm, left leg vs right leg. Hugely useful for spotting the asymmetries that come from years of one-sided dominance in cleans, snatches and pistols.
Visceral fat – the metabolically dangerous fat around your organs that a low body-fat percentage on a smart scale can completely hide.
Bone mineral density – vital for HYROX athletes running 8km a week on hard surfaces, female athletes in any energy-restricted phase, and anyone over 40.
This is the scan that elite combat sport athletes have used to make weight cleanly. It’s the scan US high school wrestling federations rely on to certify safe minimum weight classes. And it’s the scan you should be running every 3–6 months if you actually care about whether your “cut” is shedding fat or eating your hard-won quad mass.
The use case for masters athletes is even bigger. If you’re a 45-year-old CrossFitter or training for masters HYROX, that bone density readout isn’t a vanity metric – it’s how you find out whether you’re heading towards osteopenia long before you fracture something on a box jump.
2. MSK MRI: The “Should I Scan or Should I Wait?” Decoder
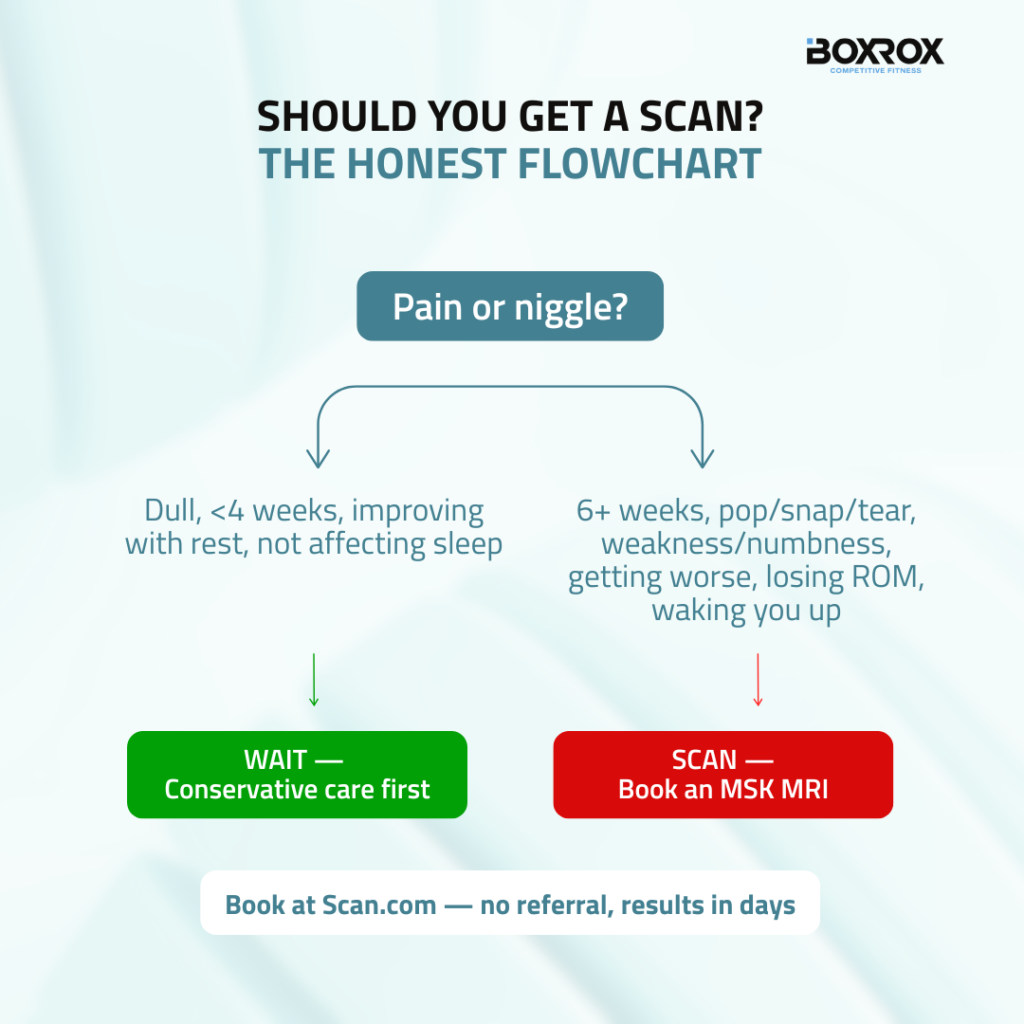
Here’s the honest framework most physios will give you when you ask whether you need an MRI:
Wait it out if: the pain is dull, hasn’t lasted longer than 2–4 weeks, improves with rest and gentle loading, and isn’t stopping you sleeping. Most rotator cuff tendinopathies, mild patellar tendinopathy, low-grade Achilles tendon issues and ordinary muscle soreness fall here. Conservative care – load management, eccentrics, mobility, smart programming – wins.
Scan it now if:
- Pain has lasted more than 6 weeks despite conservative work.
- You felt a specific pop, snap or tear during a lift or jump.
- You have weakness or numbness down a limb, not just pain.
- Pain is getting worse, not better, week-on-week.
- You’re losing range of motion you used to have.
- It wakes you up at night.
Why does this matter? Because the conditions that get worse when ignored are exactly the ones that destroy long-term training: full-thickness rotator cuff tears retract and atrophy when left, leading to muscle wasting and eventual shoulder arthritis; an Achilles partial tear that’s mistaken for tendinitis can become a full rupture; a meniscus tear that’s “trained through” becomes chronic knee osteoarthritis a decade earlier than it should.
The data on shoulders alone is striking. A 2024 MRI study covering active CrossFitters across 13 German boxes (aged 21–45) found 49% had partial supraspinatus tears, over 21% had labral lesions, and nearly 18% had biceps pulley injuries. All things you cannot diagnose from the outside. Kipping muscle-ups, ring dips, and high-volume thrusters are particularly nasty drivers.
A targeted MSK MRI through Scan.com – shoulder, knee, hip, ankle, elbow – gives you a definitive yes/no on whether what you’re feeling is something that gets better with the right rehab, or something that needs an orthopaedic opinion. Knowing which one you’re dealing with is the difference between four weeks off and four months off.
3. Spine MRI: For Everyone Who Pulls Heavy
The deadlift, the clean, the snatch, the heavy front squat, the sandbag shoulder-to-overhead in your local HYROX qualifier – your lumbar spine eats a stupid amount of compressive and shear load every week, and your default coping mechanism is usually “rub some chalk on it.”
Here’s the rule of thumb. Muscular low-back strain feels diffuse, doesn’t shoot down the leg, calms down within 2–4 weeks with smart loading, and doesn’t come with any neurological symptoms. Discogenic pain is different – sharper, often centralised, can radiate into the glute or down the leg, gets worse with axial loading (squats, deadlifts), and frequently presents with sciatica-like signals: tingling, numbness or weakness in a specific area.
If your back pain shoots into a leg, comes with numbness or pins-and-needles, lasts longer than 4–6 weeks, gets reliably worse with deadlifts or squats, or is preventing you from training in any meaningful way – you want a spine MRI. Period.
Here’s the thing nobody likes to say out loud: even CrossFit Games champions deal with this. Two-time Games winner Annie Thorisdottir collapsed before the 2014 season after an MRI revealed a bulged L5-S1 disc at the base of her spine. She couldn’t do an air squat. But getting a definitive imaging diagnosis is what allowed structured rehab and her eventual return to the podium that same year. The athletes who train blind and never get the picture taken are the ones who end up with chronic, undiagnosed back issues for the next decade.
A spine MRI doesn’t tell you to stop lifting forever. Most of the time it does the opposite — it tells you exactly what’s going on, which means your physio or strength coach can write a programme that loads you appropriately rather than guessing.
4. Cardiac: The Scan Most Athletes Are Quietly Avoiding
This is the uncomfortable one. We need to talk about it.
Functional fitness has, for two decades now, attracted exactly the kind of fit, strong, high-output people who tend to assume their hearts are fine because they can hit a sub-5 1k row. That assumption is wrong often enough that it kills people.
The 2024 CrossFit Games death of 28-year-old Serbian athlete Lazar Đukić was officially ruled a drowning during the opening swim event. But the autopsy, obtained under the Texas Public Information Act, noted cardiac enlargement with left ventricular hypertrophy – a 1.8 cm wall versus a normal 1.1–1.3 cm – consistent with “Athlete’s Heart.” The finding itself is benign. But the reason it matters is that Athlete’s Heart can look very similar on basic screening to hypertrophic cardiomyopathy (HCM), the leading cause of sudden cardiac death in young athletes worldwide. The difference between “benign physiological adaptation” and “potentially lethal cardiomyopathy” cannot be made on a stethoscope alone. It needs imaging.
The screens that matter for a serious functional fitness athlete, especially over 35 or with any family history:
Stress echocardiogram – looks at how the heart pumps under exertion. A good first-line screen.
Cardiac CT / coronary calcium score – for older athletes, the early-detection tool for silent coronary artery disease.
Cardiac MRI – the gold standard for distinguishing physiological athlete’s heart from genuine cardiomyopathy, plus picking up myocarditis and other structural issues.
If you’re over 40, have a family history of sudden cardiac death, or you’ve ever had a symptom that made you pause mid-WOD – dizziness, palpitations, unusual shortness of breath, chest discomfort – this is not the scan you put off until next year.
5. Full-Body MRI: The Longevity Play
This is the bit that’s gone mainstream over the last 24 months, and you can credit the longevity movement for it.
Peter Attia has been recommending whole-body MRI for early cancer detection since 2015 and co-founded the whole-body MRI startup Biograph. Bryan Johnson uses imaging as part of his Blueprint protocol. The longevity and proactive health optimization community has pushed this from “fringe biohacker” territory into something genuinely practical.
The case for full-body MRI is straightforward: it’s a radiation-free, single-session screen of the brain, chest, abdomen, pelvis and major vessels that can pick up tumours, aneurysms and structural anomalies years before they become symptomatic. There are caveats — the American College of Radiology has not endorsed it as a population-screening tool, and false positives that lead to anxiety and unnecessary follow-up are a real concern. So this isn’t a blanket recommendation for everyone.
But for high-performing athletes who already optimize sleep, training, blood panels and HRV, full-body MRI is increasingly part of the toolkit. The mindset shift it represents – from reactive medicine (“I’ll see a doctor when something breaks”) to proactive health (“I’ll find problems before they become problems”) – is the same mindset shift that took CrossFit from fringe to mainstream.
If you can afford it, do it every 2–3 years from your 40s onwards, ideally alongside annual bloodwork and a DEXA. That’s the protocol the longevity world has converged on.
How to Actually Pull the Trigger
You don’t need a referral. You don’t need to wait six weeks on a list. You don’t need to fight your insurance company.
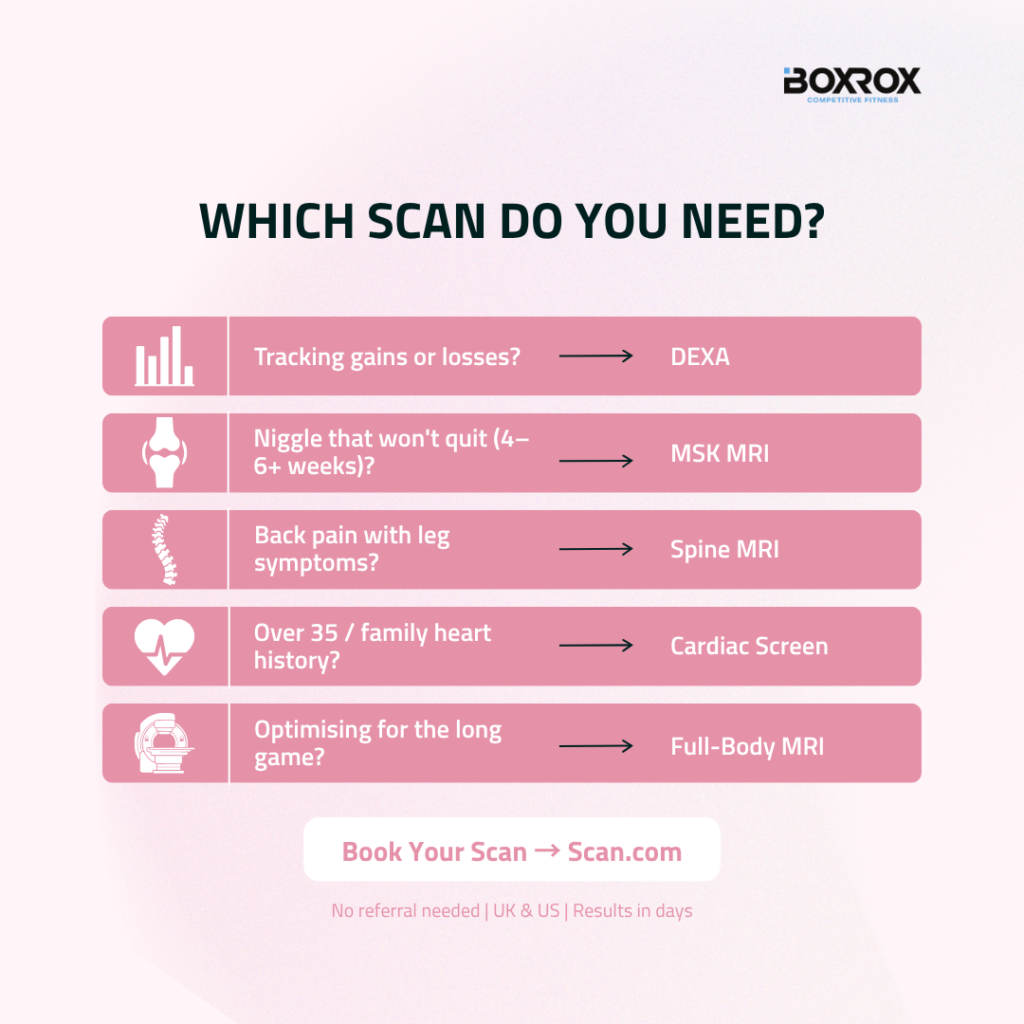
Pick the scan that matches the problem you’re trying to solve:
- Tracking gains or losses? → DEXA.
- Niggle that won’t quit after 4–6 weeks? → Targeted MSK MRI.
- Back pain with leg symptoms or refusing to resolve? → Spine MRI.
- Over 35, masters competitor, or any family heart history? → Cardiac screen.
- Optimising for the long game? → Full-body MRI.
Head to Scan.com, choose your scan type and location, and book online in minutes. The clinician call follows. The scan happens. The report lands in your inbox in days, not months.
Your training deserves data, not guesses. Your body deserves answers, not “let’s wait and see.” And your future deserves an athlete who’s still pulling 1.5x bodyweight off the floor at 60 because they took five minutes to look inside the engine at 35.
Train hard. Scan smarter. See you in the box.
This article is sponsored by Scan.com. Content is for general information and is not a substitute for advice from a qualified medical professional. If your symptoms are severe, worsening, or making you worried, seek urgent medical advice through your local emergency service or NHS 111 / 911.
References
- Feito, Y. et al. “A 4-Year Analysis of the Incidence of Injuries Among CrossFit-Trained Participants.” Orthopaedic Journal of Sports Medicine, 2018. — https://pmc.ncbi.nlm.nih.gov/articles/PMC6201188/
- NHS England. “Diagnostic Waiting Times and Activity Report — January 2026.” — https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2026/03/DWTA-January-2026-Report_42P3N.pdf
- “Shoulder pathologies in CrossFit: a magnetic resonance imaging study of 51 cases.” Journal of Sports Medicine and Physical Fitness, 2024. — https://pubmed.ncbi.nlm.nih.gov/38445843/
- Thorisdottir back injury coverage. CrossFit Games Media, 2013 / Sports Illustrated, September 2014. — https://games.crossfit.com/article/thorisdottir-sidelined-back-injury
- Đukić autopsy findings. The Barbell Spin, 2024. — https://thebarbellspin.com/crossfit-games/autopsy-of-lazar-dukic-finalized-no-signs-of-cardiac-arrest/
- Jafari, H. et al. “Myocarditis in Athletes Recovering from COVID-19: A Systematic Review and Meta-Analysis.” International Journal of Environmental Research and Public Health, 2022. — https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8998516/
- Nuffield Trust. “Diagnostic test waiting times.” — https://www.nuffieldtrust.org.uk/resource/diagnostic-test-waiting-times
- Scan.com — About Us. — https://scan.com/about-us









